

If you’ve become unplugged from the evolving headlines surrounding Elon Musk’s brain-computer interface (BCI) startup, Neuralink, here’s a recap:
- In January, Neuralink implanted their first participant, Noland Arbaugh, with the N1 implant at Barrow Neurological Institute in Phoenix, AZ. According to Neuralink’s website, “The N1 Implant records neural activity through 1024 electrodes distributed across 64 threads. These highly-flexible, ultra-thin threads are key to minimize damage during implantation and beyond.”
- In mid-March, Noland was announced to the world via livestream by Neuralink (on Musk’s platform, X), playing games using his implant.
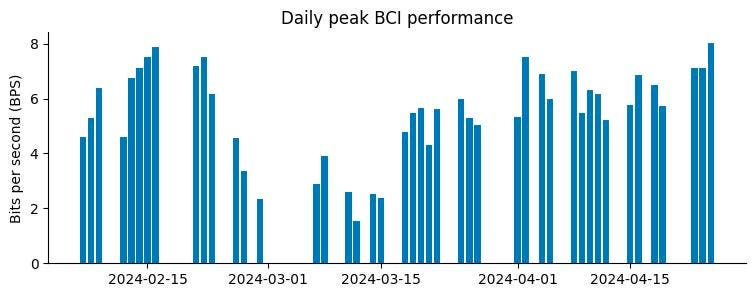
- On May 8, a company blog post revealed that in the weeks following the surgery, “a number of threads retracted from the brain, resulting in a net decrease in the number of effective electrodes.” (see dip in the chart above.) Despite this malfunction, the company was able to restore full function through augmenting software, without needing additional surgical correction of the implant’s wires.
- The next day, The Wall Street Journal ran a story, speculating possible reasons why the implant might have malfunctioned, and suggesting that it was their initial inquiries to Neuralink that led to publication of the blog post. A Wired piece the same day explained various mechanical differences in today’s commercially oriented (but pre-market) BCI devices, citing external competitors and experts who pointed to the importance of durability as a key design attribute in this technology.
- On May 15, Reuters reported that Neuralink has known about the wires’ retraction issues for years, going back to their animal testing phase, citing five anonymous sources speaking behind confidentiality agreements. One of these sources said that the FDA’s initial rejection of Neuralink’s application to begin human trials included safety concerns about the implant’s threads.
- On May 20, another WSJ article reported that 85% of the threads had retracted, that the next implant will be implanted 8 millimeters deep (compared to 3 to 5 millimeters in Arbaugh), and that the FDA had greenlit Neuralink’s recruitment for their second patient.
- On May 22nd, Arbaugh spoke with Wired again to share his perspective. When asked whether he’d known that wire retraction was possible, he said, “I didn’t have any knowledge that it was possible. I don’t think they saw it in any of the animal trials. I had heard that it had maybe happened in one of the monkeys but that it was much different. It was never anticipated that it would happen in me.” He later stated, “It seems like the threads have stabilized, and even some that were pulled out of my brain had found their way back in.”
Since then: More interviews, more media coverage, more speculation, more questions. With Musk there’s always more. But let’s stop the tape here and reflect.
In the span of two weeks: One company blog post, five anonymous sources, four great reporting teams (among many others), one sociable participant and one silent federal agency have turned this story – about a safety trial for a medical device – into a web-wide drama with more questions than answers.
The most important detail: Arbaugh appears to be okay. But instead of moving on, the neurotech industry might consider this a teachable moment for reflection.
The question isn’t “What went wrong?” but “What can be learned from this?”
A caveat: The retraction issue that happened is based on Neuralink’s specific product design, wherein the threads shown below came loose. Other companies’ BCIs use different means of implanting electrodes onto or into the brain.
How can the stewards of BCI’s fast-approaching future use this episode to improve safety, optimize access and strengthen the public’s trust in this technology?
What Can Neuralink Do Differently Moving Forward?
Nobody expects much to change. Musk has a well-documented distrust and disdain for both media and the government, and a penchant for controlling the narrative. But as a company, Neuralink has shown a glimmer of willingness to respond to media and regulatory criticism on their blog, albeit indirectly, after the fact, and stopping well short of a mea culpa.
I may be in the minority here but I thought their May 8 blog post was a good first response: direct, succinct, practical. A technical solution to a technical problem.
The issue is that it didn’t go far enough. BCI are not nuts and bolts. They are a human-powered technology. This is a human trial. Arbaugh is a human being.
So, beyond the mechanical solution of deeper implants, what did they learn from this incident, their very first involving an actual person? What changes are they exploring to improve subsequent human trials? How will they evolve to live up to their stated culture, where “open communication and collaboration underpin our commitment to transparency and championing the best ideas, regardless of where they come from” ?
Instead of hazarding such self-awareness, Neuralink has remained characteristically opaque on the matter at hand so far, abstaining from media comments and diverting attention instead towards their recruitment of a second US patient, advances in global trials, and ongoing product development related to restoring vision and touch via BCI.
The company has also issued a new “technical challenge” whose convenient timing will help shift the narrative. And so it goes.
But it’s not too late. In fact it’s still quite early. Let’s keep an eye on that blog.
Can We Improve Informed Consent for Experimental Trials?
Arbaugh clearly did not understand retraction was a risk. Neuralink clearly did.
The particular details of Arbaugh’s pre-trial onboarding will likely remain private. But what can be done to improve this kind of information asymmetry for other people?
Those enrolling in new BCI trials are going where none (or few) have gone before. Informed consent requires that participants are notified of any “reasonably foreseeable risks.”
Far beyond BCI, informed consent is a bigger can of worms than the Dune sequel.
It’s ripe for reform: “the subject of discussion for at least 3 decades, with a consistent consensus throughout this time that these documents are too difficult to read, too complex, and too long and, as a result, frequently fail to facilitate truly informed consent by study participants.”
Informed consent isn’t overseen by the FDA (which seemed to know about the risk of wire retraction in N1 implants,) but by an entirely separate office within HHS called the Office of Human Research Protection. The OHRP chooses when to exercise regulatory oversight. But STAT’s recent crackerjack reporting on an unrelated and ongoing informed consent debacle at Mt. Sinai, showed how this office simply ignored the FDA’s email “alarm bells,” despite repeated breakdowns in protecting patients from medically dubious brain biopsies that one neurosurgeon described as “almost Geneva Convention stuff.”
In the years ahead, as companies develop and test BCIs, each with different device designs and implantation protocols, brain-related studies could become a textbook example of the urgent need to improve the informed consent process at the federal level to protect people’s most inviolable core of autonomy, identity, and consciousness. Incorporating accessible language suitable for every education level, new formats and tools and better avenues to ask questions may ensure more risks are understood without the need for an attorney.
To be clear: This goes far beyond Neuralink or any BCI company. While trial participants aren’t quite flying blind, enrolling in trials for experimental brain implantation represents a complex choice amidst strongly vested interests. As Arbaugh put it:
“…I’m a quadriplegic, and all I really have is my brain. So letting someone go in there and mess around, it’s a big commitment. If something goes wrong, that’s kind of it for me. But I knew I wanted to help out, and I didn’t want to let my fears get in the way of that. The second thing that gave me pause was that I didn’t know if I wanted to be the first one to get this in my brain if anything would go wrong with the implant. What if it breaks or stops working and I only have it for a day, a week? I thought maybe someone else should get it first, and I’ll get the better version of it.”
As per his wishes above, how can subsequent patients in each clinical trial be better informed by the experience of the first? The BCI Pioneers Coalition exists to ensure those in Arbaugh’s position don’t have to shoulder the responsibility of educating new trial participants about risks and benefits of an investigational study. But not all participants in BCI trials are aware of this resource, or other avenues of support, before they join a trial.
What Counts as “Promotion” under IDE?
As per the BPS graph above: On March 20, when Neuralink introduced the world to Arbaugh via Musk’s own social media platform, they had known about the wire issue for barely two weeks. Yet, rather than pausing, reflecting, monitoring, they began filming.
It’s not unheard of for the first patient in an FDA-regulated safety trial to become a PR project by the trial sponsor. But why doesn’t this behavior count as “promotion” under the FDA’s rules for Investigational Device Exemption (IDE) studies?
As per the FDA’s IDE guidelines, “Sec. 812.7 Prohibition of promotion and other practices. A sponsor, investigator, or any person acting for or on behalf of a sponsor or investigator shall not: (a) Promote or test market an investigational device, until after FDA has approved the device for commercial distribution.”
The FDA is operating in a pre-social media world, a pre-Elon-Musk-world, and a pre-Elon-Musk-owning-social-media-world.
To be fair, the agency isn’t responsible for anticipating these kinds of unprecedented situations or historically powerful actors. But now that it has happened – is still happening – it’s no longer unprecedented. Is this a regulation, or a suggestion?
Agency leadership is legally required to “decline to comment” on such matters, but even so: How, when, or will they clarify, adapt or enforce their policies?
Is Promoting BCI Really a Patient’s Job?
Arbaugh has been admirably vocal about his desire to contribute to advancing BCI. By all indications, Neuralink has been there for him and his family in major ways, before, during, and after implantation. But surely the combined role of highly visible spokesman and trial research subject is a lot of pressure for one person.
The patient advocates I’ve spoken to are in alignment that awareness and education – particularly in engaging the general public – are a key priority for BCI. Dystopian ‘mind control’ narratives do not reflect reality; the story needs correcting.
But first comes safety, then comes advocacy.
A practical question for the years ahead: Is there a difference between promoting or test marketing an investigational device, and recruiting for clinical trials and patient registries, vis-a-vis dedicated websites, social media, and beyond?
Neuralink, whose registry has reportedly recruited more than 1,000 patients, is now expanding their trials into Canada and Britain. Arbaugh’s words and likeness blanket the website. He seems happy to serve as unpaid ambassador, despite the centripetal forces of a media carousel that benefits the company and their ongoing trial far more than him.
This grey area isn’t entirely unique to Neuralink. BCI exists in the public imagination already. Startups are wading into this as they commercialize.
Rival Synchron, who launched their registry this year in preparation for a larger scale clinical trial, has also shared their participants’ stories on national television and social media, albeit without fixing a permanent spotlight onto them. Every company taking BCI through the FDA will need to recruit patients and, to an extent, build trust from the public.
As neurotechnology climbs the hype cycle, one can forget that “BCI” are not just a trending topic, but medical devices designed to remain inside people’s bodies for years. The “moral entanglements” between research teams and trial participants don’t stop at the end of these multi-year trials. Considerations for the long tail that follows – ongoing clinical care guidelines, public-private responsibilities to patients and the economic implications for coverage and reimbursement – are just emerging.
As the FDA’s new implantable BCI collaborative community convenes this year, patient advocacy groups will fortunately be at the table to guide the field. Beyond public education and messaging, their leadership will be critical to balance corporate interests in brand building, clinical interests in trial recruitment, and regulatory interests in advancing innovative treatments safely.
Good News for People Who Love Bad News
When the most powerful private and public stakeholders involved in a story don’t comment, some people start speaking off the record, others speculate, and some like Arbaugh pick up the slack and take it on themselves.
Leaders in my neurotech community are in active discussion about how best to discuss such highly technical, highly-regulated, still-developing news with media and the general public.
Despite the musk of intrigue and drama, I believe this story is good news. Here’s why.
- Noland Arbaugh is okay. Despite the wire retraction, his BCI works great, his sponsor has proven adaptive and creative, and he’s still able to do what he enjoys. With his optimism and grace under pressure he has handled this situation admirably. I hope he doesn’t burn himself out with media. I’d gently suggest that finding support outside of Neuralink is good idea.
- If this much critical discussion about BCI can emerge from a single story, thanks to a combination of sharp reporting, willing confidants, and yes, a polarizing celebrity billionaire founder, that is a great outcome. Hopefully all stakeholders are able to absorb some lessons and implement some changes – even if they don’t want to (or cannot legally) talk about it.
- This bodes well for other BCI companies, present and future, as a reminder to prioritize methodical and prudent compliance with safety studies over speed to market and public optics. In the long term, this underscores that patients will need multiple options so they aren’t forced to choose one product (or registry.) Investors should feel confident in this stage of BCI’s regulatory journey, even if revenue remains years away.
- Neuralink has seemingly learned critical product optimization and made adjustments on the fly. This is what successful startups do. Hopefully, there are no additional malfunctions involving human subjects. Let’s wish them luck, while holding them to a higher standard of excellence in clinical trials as a highly visible leader in this nascent field.
Read the full article here